
Table of Contents
- 1 What Is a Sebaceous Cyst?
- 2 Epidemiology and Incidence of Sebaceous Cysts
- 3 Genetics and Molecular Biology of Sebaceous Cysts
- 4 Histopathological Features and Diagnosis
- 5 Causes of Sebaceous Cysts
- 6 Symptoms of Sebaceous Cysts
- 7 Diagnosis and Examination of Sebaceous Cysts
- 8 Treatment Options for Sebaceous Cysts
- 9 Post-Treatment Course and Prognosis
- 10 Complications and Precautions
- 11 Surgical Costs for Sebaceous Cysts
- 12 Frequently Asked Questions About Sebaceous Cysts
- 12.1 Q: Can sebaceous cysts resolve on their own?
- 12.2 Q: What is the difference between a sebaceous cyst and an epidermoid cyst (atheroma)?
- 12.3 Q: In cases of multiple sebaceous cysts, is there a possibility of a hereditary disease?
- 12.4 Q: What is the recurrence rate after surgery?
- 13 References

What Is a Sebaceous Cyst?
A sebaceous cyst is a benign cystic tumor arising from the sebaceous glands, which are responsible for secreting sebum [1,2]. Formally referred to as a “sebaceous cyst,” it is classified as a type of skin adnexal tumor [1,11]. Sebaceous cysts are a relatively uncommon skin condition, estimated to account for approximately 1–2% of all skin tumors [2,14].
Solitary sebaceous cysts occur sporadically, whereas multiple cysts are strongly associated with hereditary diseases [4,5,7]. In particular, hereditary tumor syndromes such as Muir-Torre syndrome are known to feature multiple sebaceous tumors as a characteristic cutaneous manifestation [4,5,9,10].
Epidemiology and Incidence of Sebaceous Cysts
Sebaceous cysts are a relatively uncommon condition, with an estimated annual incidence of approximately 0.5–1 case per 100,000 population [2,14]. There is little difference in incidence between males and females, and while they occur across a wide age range, onset in adulthood is more commonly observed [1,2].
Predilection sites include areas rich in sebaceous glands: the anterior chest (approximately 40%), the axillae (approximately 25%), and the neck (approximately 20%) [14]. They may also develop on the face and scalp, although secondary development from nevus sebaceus should be considered at these locations [15,17].
Genetics and Molecular Biology of Sebaceous Cysts
Solitary sebaceous cysts are typically sporadic, while genetic factors play an important role in multiple sebaceous cysts [7]. Mutations in the keratin 17 (K17) gene, which follow an autosomal dominant inheritance pattern, have been reported; these mutations are thought to cause abnormal differentiation of the sebaceous glands [7].
In Muir-Torre syndrome, mutations in DNA mismatch repair genes (MSH2, MLH1, MSH6, PMS2) give rise to a characteristic combination of sebaceous tumors and visceral cancers, particularly colorectal cancer [4,5,9,10]. In this syndrome, sebaceous tumors—including sebaceous cysts—serve as important cutaneous warning signs [5,13].
Histopathological Features and Diagnosis
The histopathological features of sebaceous cysts are characterized by a cyst wall composed of mature sebaceous cells and sebum-like material within the cyst cavity [2,12]. Immunohistochemically, positivity for sebaceous markers such as adipophilin and perilipin-1 is useful in confirming the diagnosis [2,12].
The most important differential diagnosis is distinction from an epidermoid cyst (atheroma) [1,3]. Epidermoid cysts characteristically display a central punctum (umbilication), whereas sebaceous cysts do not [1]. The tendency toward multiple lesions is also a helpful distinguishing feature [14].
Causes of Sebaceous Cysts
Sebaceous cysts are thought to develop as a result of obstruction of the sebaceous gland opening or duct, which prevents normal secretion of sebum [1,2]. In solitary cases, the condition is non-hereditary, and secondary ductal obstruction due to trauma or inflammation is often identified as the cause [1].
In multiple sebaceous cysts, genetic factors are important; mutations in the keratin 17 (K17) gene with autosomal dominant inheritance have been reported [7]. These mutations lead to abnormal differentiation of the pilosebaceous unit, resulting in multiple sebaceous cysts [7].
Sebaceous cysts may also develop secondarily from nevus sebaceus [15,17]. In such cases, hormonal changes after puberty may activate the nevus sebaceus, with the potential development of various sebaceous tumors (including sebaceous cysts, sebaceous adenomas, and sebaceous carcinomas) [15,17].
Symptoms of Sebaceous Cysts
Sebaceous cysts commonly develop in areas rich in sebaceous glands, including the anterior chest, axillae, and neck [1,14]. They present as skin-colored to pale yellow, hemispheric, elevated nodules with a smooth surface and mobility on palpation [1,2].
The most characteristic feature of sebaceous cysts is their tendency toward cluster formation, with multiple cysts developing in close proximity [14]. Although solitary cysts occur, new cysts frequently appear in the surrounding area over time [14].
Sebaceous cysts are generally asymptomatic; however, if the cyst wall ruptures and inflammation occurs, swelling and pain may develop [1,3]. Rupture allows sebum-like contents to leak into the surrounding tissue, where inflammatory granulation tissue may form [1].
An important distinguishing feature from epidermoid cysts (atheromas) is the absence of a central punctum (umbilication) in sebaceous cysts [1]. The tendency toward multiple lesions is also a useful finding in differentiation from epidermoid cysts [14].
Diagnosis and Examination of Sebaceous Cysts
Diagnosis of sebaceous cysts is primarily based on clinical features [1,11]. On inspection, the lesion appears as a skin-colored to pale yellow hemispheric nodule; on palpation, it is felt as a soft, elastic, and mobile mass [1].
Imaging studies such as ultrasound can depict the lesion as a cystic mass with a uniform hypoechoic area internally [16]. On MRI, the lesion characteristically shows signal intensity equivalent to fat on T1-weighted images, and high signal intensity on T2-weighted images as well [16].
Histopathological examination is required for a definitive diagnosis, with confirmation of a cyst wall composed of mature sebaceous cells being essential [2,12]. Immunohistochemical examination demonstrates positivity for sebaceous markers such as adipophilin and perilipin-1 [2,12].
In cases of multiple sebaceous cysts, the possibility of hereditary tumor syndromes such as Muir-Torre syndrome should be considered, and it is important to take a thorough family history and consider genetic testing [4,5,13].
Treatment Options for Sebaceous Cysts
Surgical excision is the definitive treatment for sebaceous cysts [3,16]. Complete removal including the cyst wall helps reduce the likelihood of recurrence [3,16]. Surgery is performed under local anesthesia, with the incision line determined according to the size and location of the cyst [16].
Aspiration of the cyst contents provides temporary reduction, but because the cyst wall remains, recurrence is common [3]. Therefore, surgical excision is generally recommended as the preferred approach even when symptom relief is the primary goal [3,16].
For multiple sebaceous cysts, the treatment plan is determined based on a comprehensive assessment of both cosmetic and functional considerations [14]. Since it is often not practical to remove all cysts at once, a staged approach is commonly adopted according to the patient’s preferences and the severity of symptoms [14].
Carbon dioxide (CO₂) laser treatment is another option; however, since complete removal of the deep cyst wall may not always be achieved, the risk of recurrence must be carefully considered when determining its suitability [16].
Post-Treatment Course and Prognosis
With appropriate surgical excision, the prognosis is generally favorable; the recurrence rate following complete removal has been reported to be below 5% [3,16]. Post-operative complications are uncommon, and when they do occur, they tend to be mild, such as temporary swelling or minor discomfort [16]. For multiple sebaceous cysts associated with hereditary conditions such as Muir-Torre syndrome, regular dermatological follow-up and general medical screening (including colorectal cancer screening) are important [4,5,13].
Complications and Precautions
The main complication of sebaceous cysts is inflammation resulting from rupture of the cyst wall [1,3]. Rupture causes sebum-like contents to leak into the surrounding tissue, triggering a foreign-body inflammatory reaction [1].
In cases of multiple sebaceous cysts, the possibility of hereditary tumor syndromes such as Muir-Torre syndrome should always be kept in mind [4,5,13]. In this syndrome, sebaceous tumors may present as a warning sign of colorectal or urogenital cancer, making early detection and treatment particularly important [5,10].
Sebaceous cysts arising in association with nevus sebaceus carry a risk of malignant transformation (sebaceous carcinoma) after puberty, and regular monitoring is therefore necessary [15,17,18]. If rapid enlargement or ulceration is observed, a tissue biopsy should be performed promptly [17,18].
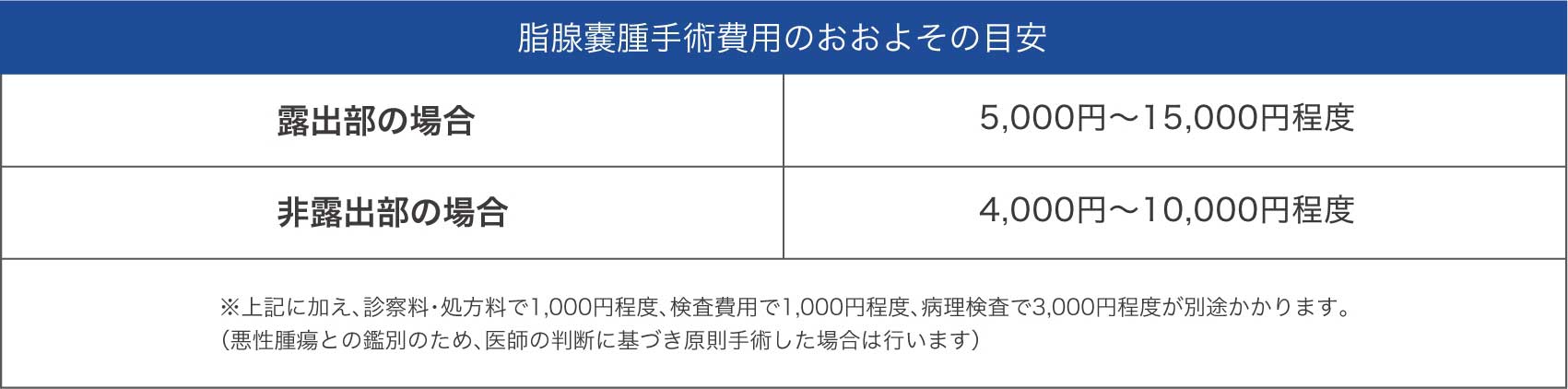
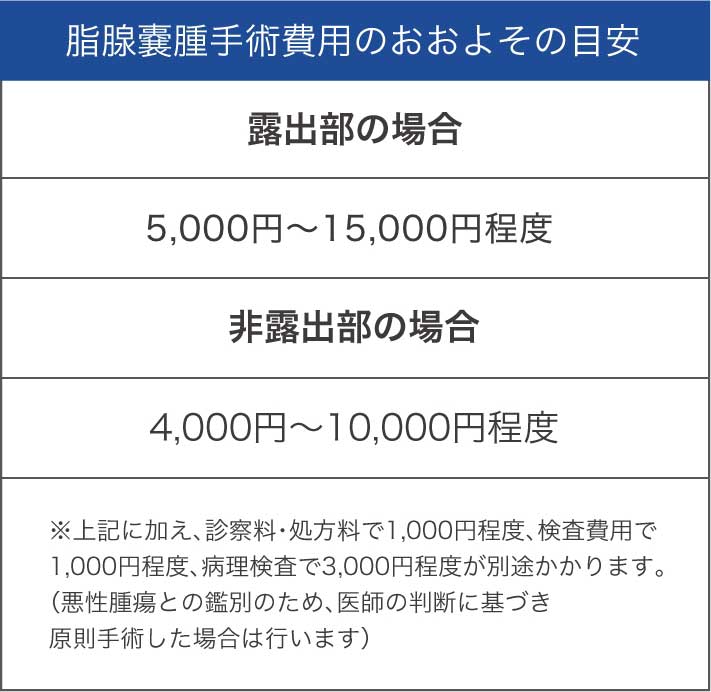
Surgical Costs for Sebaceous Cysts

Frequently Asked Questions About Sebaceous Cysts
Q: Can sebaceous cysts resolve on their own?
A: Sebaceous cysts rarely resolve on their own [1,3]. As long as the cyst wall remains, contents will re-accumulate, leading to recurrence [3]. Surgical excision is required for definitive treatment [3,16].
Q: What is the difference between a sebaceous cyst and an epidermoid cyst (atheroma)?
A: The most important distinguishing feature is that epidermoid cysts characteristically have a central punctum (umbilication), whereas sebaceous cysts do not [1]. In addition, sebaceous cysts tend to present as multiple lesions, which is another useful finding for differentiation [14].
Q: In cases of multiple sebaceous cysts, is there a possibility of a hereditary disease?
A: Multiple sebaceous cysts may be associated with hereditary tumor syndromes such as Muir-Torre syndrome [4,5]. In such cases, there is an elevated risk of concurrent visceral cancers such as colorectal cancer, and genetic counseling and consideration of genetic testing are recommended [5,13].
Q: What is the recurrence rate after surgery?
A: When complete excision including the cyst wall is performed, the recurrence rate is reported to be below 5%, reflecting a favorable outcome [3,16]. However, incomplete excision or aspiration alone is associated with a higher likelihood of recurrence, which is why appropriate surgical treatment is important [3].

References
- 1. Japanese Dermatological Association, ed. Dermatology, 11th Edition. Bunkodo, 2018.
- 2. Fernandez-Flores A, Saeb-Lima M, Cassarino DS. Histopathology of sebaceous neoplasms. Am J Dermatopathol. 2009;31(5):440–451.
- 3. Zuuren EJ, Fedorowicz Z, Arents BWM. Interventions for sebaceous cysts. Cochrane Database Syst Rev. 2014;(12):CD007951.
- 4. Ponti G, Luppi G, Losi L, et al. Muir-Torre syndrome and MSH2 gene alterations: a not uncommon association in hereditary nonpolyposis colorectal cancer families. Hum Mutat. 2005;26(6):546–553.
- 5. Schwartz RA, Torre DP. The Muir-Torre syndrome: a 25-year retrospect. J Am Acad Dermatol. 1995;33(1):90–104.
- 6. Japanese Society of Plastic and Reconstructive Surgery, ed. Plastic Surgery, 4th Edition. Kokuseido Publishing, 2017.
- 7. Lisle A, Mosier M, Kandamany N. Multiple sebaceous cysts and the keratin 17 gene mutation: a case report. Dermatol Online J. 2008;14(1):7.
- 8. Harii K, Hashimoto K, eds. NEW Dermatology, 3rd Edition. Nakayama Shoten, 2018.
- 9. Smith KJ, Skelton HG 3rd, Lupton GP, et al. Sebaceous carcinoma and the Muir-Torre syndrome. J Cutan Pathol. 1995;22(4):378–385.
- 10. Akhtar S, Oza KK, Khan SA, Wright J. Muir-Torre syndrome: case report of a patient with concurrent jejunal and ureteral cancer and a review of the literature. J Am Acad Dermatol. 1999;41(5 Pt 1):681–686.
- 11. Japanese Dermatological Association. “Clinical Practice Guidelines for Skin Tumors, 2nd Edition,” 2015.
- 12. Bowen AR, LeBoit PE. Sebaceous neoplasms of the skin. Am J Dermatopathol. 2005;27(4):315–326.
- 13. Shalin SC, Lyle S, Calonje E, Lazar AJ. Sebaceous neoplasia and the Muir-Torre syndrome. Pathology. 2010;42(3):223–230.
- 14. Editorial Committee of the Japanese Journal of Dermatology. “Diagnosis and Treatment of Sebaceous Cysts.” Jpn J Dermatol. 2017;127(3):543–558.
- 15. Kossard S, Epstein EH Jr, Cerio R, et al. Basal cell carcinoma and sebaceous hyperplasia in nevus sebaceus: a morphologic study of 99 cases. J Am Acad Dermatol. 1994;30(3):373–378.
- 16. Robinson JK, Hanke CW, Siegel DM, et al. Surgery of the Skin: Procedural Dermatology, 3rd Edition. Elsevier, 2015.
- 17. Kazakov DV, Kutzner H, Rutten A, et al. Carcinomas arising in preexisting sebaceous nevus: a clinicopathologic study of 75 cases. Am J Surg Pathol. 2007;31(11):1628–1636.
- 18. Miller CJ, Ioffreda MD, Billingsley EM. Sebaceous carcinoma, ocular adnexa: a review of 14 cases. Dermatol Surg. 2001;27(1):93–96.
- 19. Harvey RG, Harman KE, Morris SD. Multiple steatocystomas and hidrocystomas: the complete spectrum of sebaceous differentiation in organoid naevi. Br J Dermatol. 2001;144(4):886–890.
- 20. Weiss SW, Goldblum JR. Enzinger and Weiss’s Soft Tissue Tumors, 6th Edition. Elsevier, 2014.




